This article is part of a larger work.
Return to the table of contents | Go to the next section
Rationale for the Use of Qualitative Research
The rationale for applying the qualitative, rather than the quantitative, method of research on fathers’ experience of perinatal loss was that few studies have thoroughly studied this topic. In fact, an abundance of the literature has focused on the mother's grief following perinatal loss. When studies have looked at fathers, they have used the same measures for mothers as they have used for the fathers. There is some evidence that fathers may have a qualitatively different grief response to this loss than mothers. For instance, Vance, et al. (1995) found that when adding a measure of alcohol ingestion to the more typical measures of grief, depression and anxiety, men had just as much distress as their female counterparts. Thus, we can conclude the indices typically used to measure grief reactions of mothers following perinatal loss may not fully capture the grief in quantitative studies are not yet measuring, so this dissertation aimed to gain a more thorough understanding of the fathers' experience of perinatal loss and identify pertinent psychological themes in these men. An interview, projective instruments, and the Perinatal Grief Scale allowed the researcher to explore the issues surrounding perinatal loss and fathers in more depth than if a single hypothesis was tested in a quantitative study. This dissertation aimed to identify themes in men that can later be used to quantitatively measure grief in men.
Protection of Human Subjects
The informed consent forms included all regulations relevant to psychotherapy and testing, such as the limits of confidentiality, Tarasoff, and mandated child and elder abuse reporting. Confidentiality was protected by omitting names and by altering identifying information (such as profession, age, and family constellation). Audiotapes were held in strict confidence in a locked file and only supervising faculty and doctoral students involved with the project were allowed to hear the tapes. Tapes and written notes were destroyed when they were no longer needed.
As with psychotherapy and psychological testing, risks associated with this study were moderate. The semi-structured interview and the projective instruments may have triggered painful issues. The information that was discussed was naturally emotionally laden. If any participant had displayed moderate signs of distress, this researcher would have ended the interview, provided the opportunity for discussion, and given appropriate referrals. No participants, however, displayed this level of distress. In fact, four out of the it validated their experience, giving them a chance to process the loss.
Chapter IV: Results
Description of the Sample
Participants consisted of five men who had lost an infant/s due to a miscarriage, stillbirth, neonatal death, and/or Sudden Infant Death Syndrome within the last three years. Four of these men were recruited from a perinatal loss support group network, while the other man was recruited from a SIDS support group network.
Demographics.
Participants reported the following demographic information during their first meeting (See Table I). All of these men were born in the United States. Three reported that they identified as “Caucasian,” one reported that he identified as “Irish/Swedish,” and one reported that he identified as “Italian/Slavic.” Four out of the five participants identified their religious affiliation, which included Christian, Episcopalian, Protestant, and Catholic. Education levels varied: two had master’s degrees, two had bachelor’s degrees, and one had a high school diploma. Ages ranged from late twenties to middle forties. All participants were married and were employed. Socioeconomic status ranged from lower middle class to middle class.
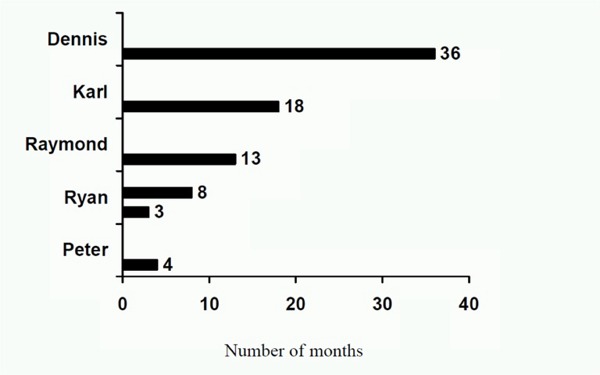
The types of losses incurred by these men varied (see Figure 1). Four of the five men lost a baby to a stillbirth, neonatal death, or SIDS. One man had two losses: a miscarriage and a stillbirth. The age of these babies at their time of death ranged from eleven weeks into the pregnancy to four months after the birth. Two of the participants had previous children at the time of the loss, and two participants have had a subsequent child since the loss. The amount of time elapsed since the loss occurred ranged from three to thirty-six months (see Figure 2).
Table I.
Demographic Information
Participant |
Religious Affiliation |
Education |
Age |
Dennis |
Christian |
High School Diploma |
36 |
Karl |
Episcopalian |
Bachelor’s Degree |
34 |
Raymond |
Protestant |
Master’s Degree |
44 |
Peter |
Not Specified |
Master’s Degree |
33 |
Ryan |
Catholic |
Bachelor’s Degree |
28 |
Figure I. Type of loss
| Participant |
Miscarriage |
Stillbirth |
Neonatal Death |
SIDS |
| Dennis |
|
X |
|
|
| Karl |
|
|
|
X |
| Raymond |
|
X |
|
|
| Peter |
|
|
X |
|
| Ryan |
X |
X |
|
|
Figure II. Time elapsed since loss
Individual Analysis
Each participant’s loss experience was unique in nature; therefore, this section provides an individual analysis of every participant based on the interviews, the PGS, the T.A.T., and the C.A.T.-H. A later section will summarize common themes among all of these men.
To fully illustrate the context of each man’s loss, these sections begin with a background that includes demographic information, the recruitment process, and a description of how the baby died. These sections then summarize the interviews, describing each participant’s experiences in chronological order. Each interview is broken down into subsections, specifying the time frame in which particular reactions occurred. The subsections for each participant vary slightly to accommodate each participant’s particular time frame. For example, it had been three years since Dennis’s (participant one’s) loss, so his interview section was separated to include his initial responses to his baby’s death, the first year of her death, and beyond the first year of her death. In contrast, Peter’s (participant four’s) baby had died only four months before the interview, so his interview description was separated into initial reactions to the loss and the first four months after her death. Ryan (participant five) had two losses; therefore, his individual analysis has separate subsections for each of his losses.
Each interview description is written in as much detail as told by the participant; therefore, the length of these sections vary. To fully illustrate each individual’s experiences, quotes have been used generously in the individual analysis.
Following the description of each participant’s interview, the scores of the PGS and a table presenting all three raters’ analyses of the T.AT. and the C.A.T.-H have been presented. An integration of all four sources of data will be discussed in Chapter five.
Participant One: Dennis
All identifying information has been changed in order to protect their confidentiality and anonymity.
Background Information
Demographic Information. Dennis, a thirty-six year-old Euro-American, Christian male, participated in the present investigation because he had a stillborn daughter, Susan, three years ago. He identifies as a Christian and works as a truck driver for a construction company. He has been married to his wife, Tammy, for twelve years. They have four living children, ages ten, eight, five, and one and a half. Tammy is currently six months pregnant.
Recruitment Process. Dennis was recruited from a perinatal loss support group in San Diego. When Dennis was “on call” for the group’s hotline, this investigator called to find out how to advertise for participants in their newsletter. After being informed of the research topic, Dennis expressed interest in participating in the study himself. During this phone conversation, he explained how he continued to miss his stillborn baby, Susan, and how her birthday was coming up. Dennis expressed excitement over the study, stating, “This is really great that you are doing this because dads are often ignored after a stillbirth.” After conducting a telephone screen to ensure that Dennis met the requirements for the study, the investigator scheduled the first meeting.
Description of the Loss. Dennis’s daughter, Susan, was stillborn three years ago. Dennis first learned that Susan had physical problems and might die when he and his wife, Tammy, attended a routine doctor’s appointment during the pregnancy (he did not specify how far along she was into the pregnancy). After doing a “high level” ultrasound, the doctor told Dennis and Tammy that Susan had several physical problems, such as Hydrocephalus as well as an inability to swallow because she did not have an esophagus. Although Susan was still alive, she was not going to live for long.
To find out if Susan’s physical problems were genetic, Tammy underwent an amniocentesis. This common procedure, which consists of drawing a sample of amniotic fluid, tests for a genetic etiology for fetal abnormalities (Dennis never reported the results of this procedure). After Dennis and Tammy got home from the procedure, Tammy felt Susan kicking and turning around a lot. The next day she did not feel her move. One week later, on Dennis’s birthday, Dennis and Tammy went to a sonogram appointment to “confirm that Susan was still alive.” However, Dennis and Tammy learned that Susan had died.
The next day, Dennis and Tammy went to the hospital to deliver Susan. Tammy had an epidural. She then “got sick” and started vomiting. Because he has a “weak stomach,” Dennis left the room. As Tammy vomited, she gave birth to Susan and yelled, “Susan’s here.” Dennis ran into the room and saw Susan lying face-down on the hospital bed.
comments powered by